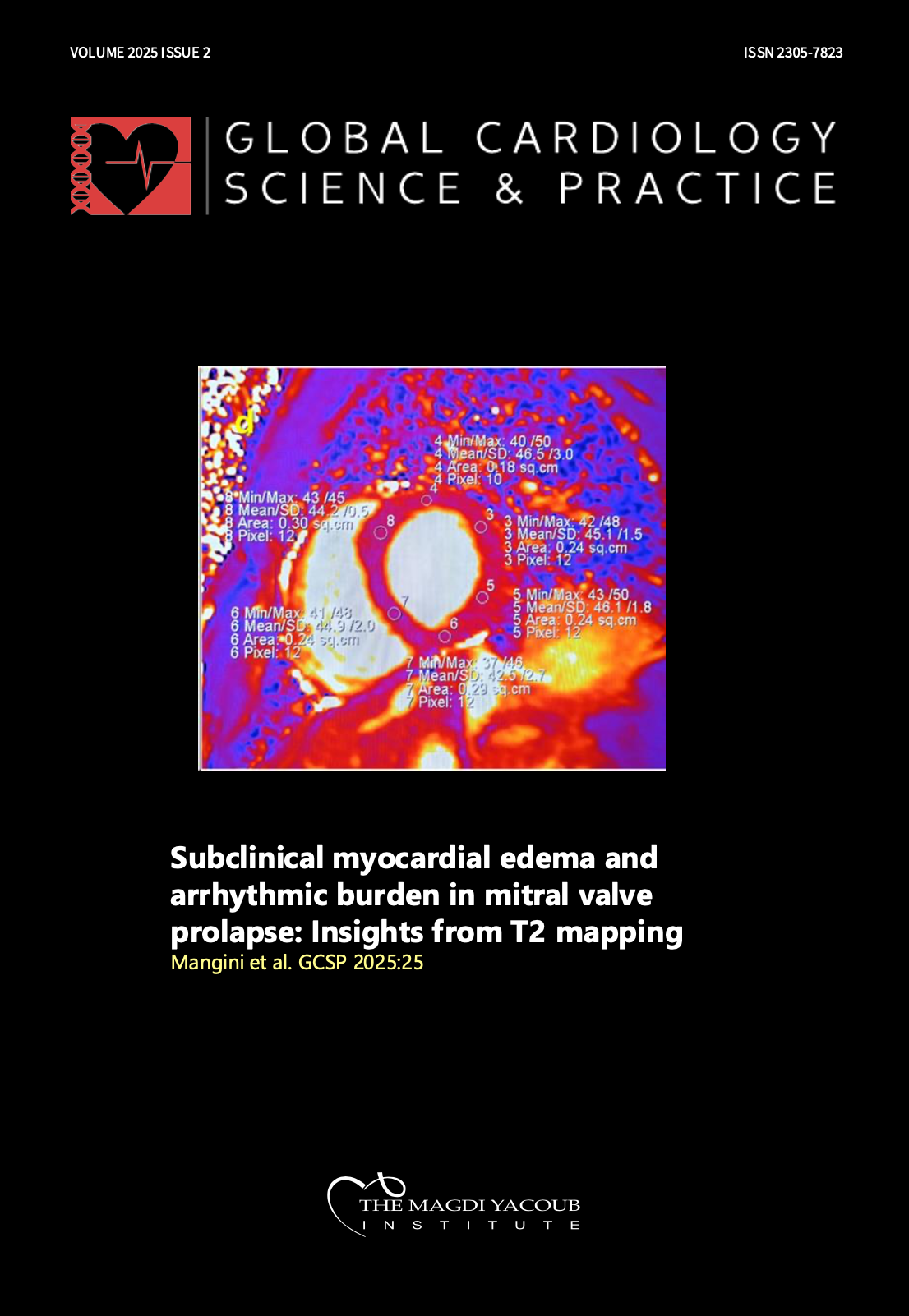
Subclinical myocardial edema and arrhythmic burden in mitral valve prolapse: Insights from T2 mapping
DOI:
https://doi.org/10.21542/gcsp.2025.25Abstract
Mitral valve prolapse is a common condition often considered benign; however, its association with arrhythmogenic risks is well established, particularly when linked with mitral annular disjunction and myocardial fibrosis. Edema often precedes fibrosis in many clinical conditions, and both edema and myocardial fibrosis are detectable in vivo using cardiac magnetic resonance. In cases of mild or chronic edema (subclinical edema), standard T2-weighted sequences may not be sufficient for identification; however, T2 mapping sequences can detect such edema. This study aims to assess whether subclinical myocardial edema identified through T2 mapping is related to arrhythmic burden in patients with mitral valve prolapse and mitral annular disjunction, even in the absence of fibrosis. Thirty-four patients underwent cardiac magnetic resonance imaging and were classified into low and high arrhythmic burden groups based on the Lown grading system. Inclusion criteria were normal myocardial signal intensity on conventional T2-weighted imaging, non- hemodynamically significant mitral regurgitation, presence of mitral annular disjunction, and absence of fibrosis. The analysis was twofold: segmental, comparing native T2 times between corresponding myocardial segments of the groups; and regional, contrasting basal segments of the lateral, inferolateral, and inferior walls, typically more affected by mitral valve prolapse, with remote myocardium within each group. Patients with higher arrhythmic burdens showed elevated native T2 times, indicating subclinical myocardial edema in the basal myocardial segments. This suggests that even without fibrosis, early myocardial alterations related to mitral valve prolapse may be related to arrhythmic risks. The clinical implications are significant, advocating the integration of T2 mapping into routine evaluations to enhance therapeutic decision making and patient outcomes. The early detection of myocardial changes may allow timely intervention and potentially modify the disease course. Further research is needed to confirm these findings and explore the utility of T2 mapping in managing mitral valve prolapse, even in patients without mitral annular disjunction.
Downloads
Additional Files
Published
Issue
Section
License
Copyright (c) 2025 Francesco Mangini, Antonio Di Monaco, Luca Sgarra, Roberto Calbi, Francesco Spinelli, Ilaria Dentamaro, Robert W.W. Biederman, Grazia Casavecchia, Matteo Gravina, Massimo Grimaldi

This work is licensed under a Creative Commons Attribution 4.0 International License.
This is an open access article distributed under the terms of the Creative Commons Attribution license CC BY 4.0, which permits unrestricted use, distribution and reproduction in any medium, provided the original work is properly cited.